Stage Three
This stage is also referred to as the stage of surgical anaesthesia.
The onset of surgical anaesthesia had previously been a relatively ‘soft’ signpost but it was clinically indispensable as this was when surgery could start. Guedel’s addition of eye signs allowed greater certainty of anaesthetic depth. Guedel’s stage three has four different planes of progressively deeper anaesthesia, during which increasingly invasive surgery could be performed.
Stage three begins with the onset of ‘automatic’ breathing (regular deep breathing with an inspiratory pause). The laryngeal response to direct stimulation of the larynx and epiglottis is abolished in this plane, however, laryngospasm in response to stimulation of abdominal organs may persist until plane four.
This stage of anaesthesia should be free of both implicit and explicit awareness.
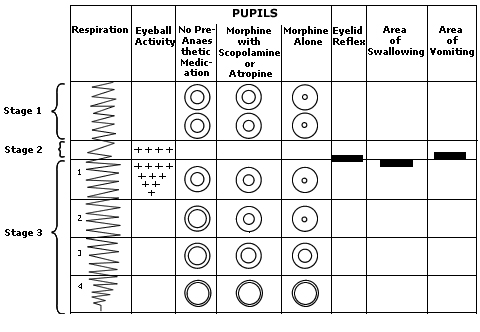
Fig 1 Stages one, two and three
'Yes, Miss Dresser, in less than two twinks the patient'll be in Paradise...Damn it girl why don't you take the mask off. You don't seem to know the difference between snoring and dying!' Anaesthesia and surgery in 1910. Dr D Zuck. Bulletin of the Royal College of Anaesthetists. November 2007. p2353-6.
Plane one: From onset of automatic respiration until eyeball movement ceases. Pupils are mid-size and central. Muscle relaxation is marginal. Touching the conjunctiva will cause blinking. This reflex disappears at the bottom of plane one.
Plane two: From cessation of eyeball movement until onset of intercostal paralysis. Pupils beginning to dilate. Pupillary response to light abolished.
Plane three: Progressive intercostal paralysis. Pupils dilating.
Plane four: From complete intercostal paralysis to onset of diaphragmatic paralysis. Tracheal tug may be observed. Laryngospasm, in response to handling of abdominal organs, is abolished.