The PCO2 of arterial blood is the most important factor in the control of breathing. If this is low, as can happen after IPPV, the patient’s respiratory drive will be reduced.
An arterial PCO2 of around 5.3 kPa will normally act as an adequate drive for respiration. In the presence of opioids, a higher value (6.0 kPa or above) may be needed because of the depression of the respiratory centre.
The capnograph, which measures end-tidal CO2 levels, will help determine if this is the cause of the hypoventilation.
CO2 levels can be allowed to rise at the end of the procedure by reducing the patient’s minute ventilation.
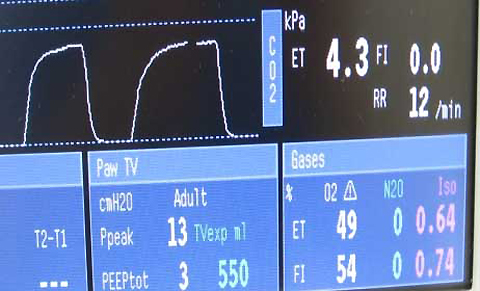
Capnograph trace