Pre-use Safety Tests
Before the epidural can be used, there are safety tests to be performed.
Before the epidural can be used, there are safety tests to be performed.
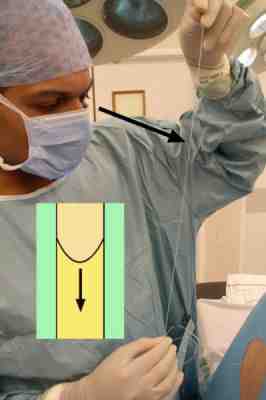
Siphon test
The catheter is held upright and a fluid level sought. If the catheter is then elevated, the fluid level should fall (see inset) as the fluid siphons in to the epidural space, which is usually under negative pressure compared with atmospheric. If the fluid column continues to rise, this may suggest subarachnoid placement. The siphon test can be reassuring, but is not mandatory.
Before the epidural can be used, there are safety tests to be performed.
Aspiration
This should be considered mandatory. The Luer connector is attached to the catheter and a syringe is used to apply negative pressure. Free and continued aspiration of clear fluid can indicate subarachnoid placement of the catheter. However, if saline has been used for loss of resistance, it is not unusual for a small amount of this to be aspirated. If there is doubt, the aspirated fluid can be tested for glucose (cerebrospinal fluid will generally test positive) or mixed with thiopentone (cerebrospinal fluid forms a precipitate). If blood is freely and continuously aspirated, this suggests intravascular placement. In this case, flushing the catheter with saline and waiting before re-aspirating is a useful test. If further fresh blood is freely and continuously aspirated, this supports intravascular placement. If only blood stained saline is aspirated, it may simply indicate aspiration of blood leaking from a traumatic insertion. In either case, if there is doubt, the catheter should not be used.

Before the epidural can be used, there are safety tests to be performed.
Test dose
This should also be considered mandatory. The bacterial filter is attached and a small dose of local anaesthetic is injected rapidly into the catheter. It should be large enough to elicit detectable effects to alert the operator to subarachnoid placement (motor block in lower limbs) or intravascular placement (circumoral paraesthesia), but small enough not to cause adverse effects such as high or total spinal block, or systemic intravascular toxicity. Considerable debate exists regarding an appropriate test dose. Bupivacaine 0.5% 3-5 ml is commonly used. Some practitioners advocate the addition of adrenaline to aid detection of intravascular placement (tachycardia being induced if the drug is given intravascularly).
