Surgical Cricothyroidotomy
Surgical cricothyroidotomy provides a definitive airway (a cuffed tube in the trachea) if tracheal intubation is not possible.
Unlike tracheostomy, it can be performed quickly and does not require a surgeon
Technique for a surgical cricothyroidotomy is:
- Extend the patient's neck fully - a rapid way to do this is to pull the patient up the trolley until the head hangs over the end. In a can't intubate can't oxygenate situation the risk of death due to hypoxia outweighs the risk of worsening a cervical spine injury
- Identify the cricothyroid membrane (Fig 1)
- Using a scalpel, make a single horizontal stab incision through the skin and cricothyroid membrane (Fig 2)
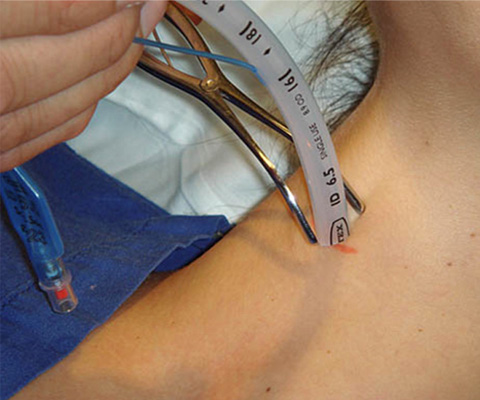
- Enlarge the hole using artery forceps or tracheal dilators, or by rotating the scalpel through 90 degrees (Fig 3)
- Insert a gum elastic bougie to 10-15cm - you may feel clicks or hold-up (Fig 4)
- If available, you can use a Rapifit connector on the end of the bougie to connect to a bag-valve-mask and re-oxygenate the patient
- Insert a size 6 cuffed tracheal or tracheostomy tube over the bougie, rotating clockwise
- Remove the bougie, inflate the cuff, check the position and ventilate
Surgical cricothyroidotomy should not be used in children - needle cricothyroidotomy with jet ventilation should be used instead.
Surgical cricothyroidotomy

Fig 1 Identifying the cricothyroid membrane
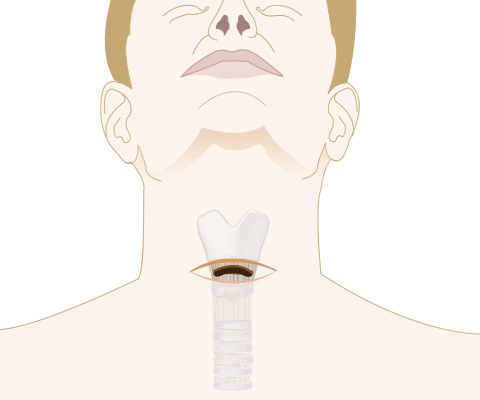
Fig 2 Horizontal stab incision

Fig 3 Spencer Wells forceps (top) and tracheal dilator (bottom)
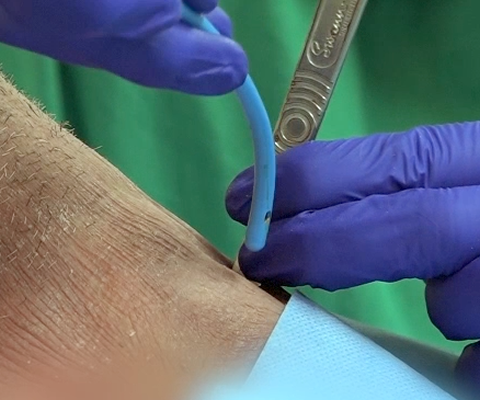
Fig 4 Elastic bougie