Adrenaline
After induction, it is a heart-stopping moment when lung compliance is so poor that ventilation fails to move any gas at all. This is a true emergency. Fortunately, it is very rare for bronchospasm of this severity to persist after treatment with adrenaline.
Blockages at any point in the breathing circuit may mimic severe bronchospasm but standard equipment checks should have identified these.
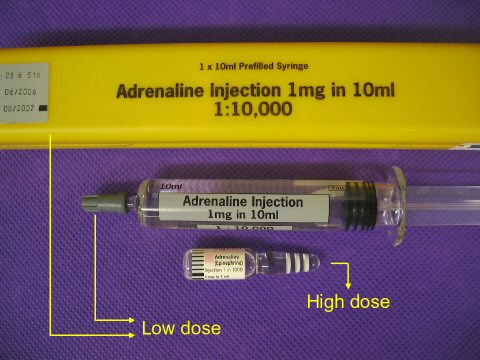
Bronchospasm of this severity may or may not be associated with anaphylaxis; in either case the treatment of choice is low dose adrenaline, starting with 50 μg-0.5 ml of 1 in 10 000 adrenaline (100 μgml), titrated to effect.
At low dose, adrenaline is mainly active at beta-adrenoceptors. This is in contrast to the high dose used in cardiac arrest, where alpha-adrenoceptor effects predominate to increase coronary perfusion by increasing the systemic vascular resistance. Severe bronchospasm requires potent beta-2 stimulation, which is provided by 50 μg increments of IV adrenaline. Once the bronchospasm is broken, a decision about continuing the case is required based on the urgency of the procedure.